Igor Bulatov писал(а):Евгений,0.03 мкг/кг эпинефрина-это всего 6 мкг/кг/мин в рассчете на 50 кг пациента.Большинство взрослых пациентов-в полтора/два раза тяжелее.6 мкг и <-не оказывает практически никакого инотропного эффекта.Особенно у пациента на байпасе и с depleted endogenous epinephrine (upregulation).
Эпидуральная болюс тест-доза эпинефрина -15 мкг,которая при внутривенном положении эпидурального катетера дает HR acceleration оf about 10-20/min у здоровых взрослых пациентов.А у кардиопациентов даже такая доза не дает никакого видимого эффекта.
Минимальная доза эпинефрина,которая может быть запрограммирована в infusion pumps,составляет 0.02 мкг/кг/мин,что ниже уровня гомосексуальной дозы.Гетеросексуальная доза эпинефрина начинается с 0.05 мкг/кг/мин при условии,что пациент не на байпасе.
Спасибо, что не стали резать.
Все же доза адреналина в 5 мкг, введенная болюсно дает тахикардию и гипертензию при условии отсутствия гиповолемии, на фоне гиповолемии при этом развивается тахикардия и гипотензия..
введение эпи без повода стронгли не рекомендуется в любом из современных учебников по кардиоанестезии:
насчет деплетед эпинефрин - категорически не согласен:
Gravlee Cardiopulmonarybypass LWW2003 писал(а):ADRENAL HORMONES
Catecholamines
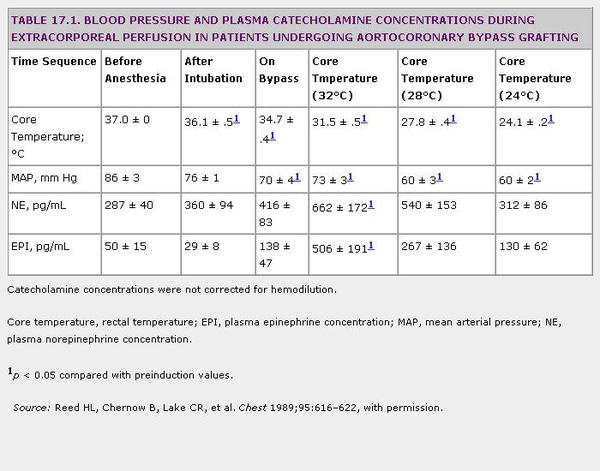
The catecholamines epinephrine and norepinephrine are products of the adrenal medulla and (in the latter case) of peripheral sympathetic and central nerve terminals. Marked elevations of plasma epinephrine and norepinephrine concentrations occurring during CPB may underlie many hemodynamic sequelae of bypass, including peripheral vasoconstriction and shifts in intraorgan blood flow (16,19–22). With hypothermia, the plasma epinephrine concentrations may increase as much as 10-fold over the pre-bypass concentrations; norepinephrine concentrations typically increase to a lesser extent (4-fold) (2,16,20,22), and deepening hypothermia attenuates these (Table 17.1). In early studies, peak increases in both norepinephrine and epinephrine occurred when the heart and lungs were excluded from the circulation (21,22). However, norepinephrine and epinephrine were found to peak at different times. In a recent study, patients undergoing cardiac surgery were randomly assigned to have CPB with mild (34°C) or moderate (28°C) hypothermia. With both bypass temperatures, peak norepinephrine concentrations were observed after release of the aortic cross-clamp and rewarming, whereas peak epinephrine concentrations were observed at the target hypothermic temperature (23). Neonates, infants, and young children, much like adults, demonstrate marked increases in catecholamine concentrations during CPB (2,24,25).
"Deeper" planes of general anesthesia (whether accomplished with larger doses of synthetic opioids, addition of a propofol infusion, higher concentrations of volatile anesthetic vapors, or addition of epidural anesthesia) significantly reduce the catecholamine concentrations of patients undergoing coronary artery bypass surgery compared with patients less deeply anesthetized (26–29). Furthermore, in critically ill neonates undergoing correction of congenital heart disease, deeper planes of general anesthesia from large intravenous doses of sufentanil not only produced lower catecholamine concentrations in response to CPB (Fig. 17.4) but also reduced mortality compared with lighter planes of general anesthesia with halothane/morphine (2). Consistent with these observations regarding anesthetic depth, infusion of propofol during bypass (4 mg/kg/hr) resulted in markedly reduced concentrations of epinephrine and norepinephrine compared with a single bolus injection of diazepam 0.1 mg/kg (27). Addition of thoracic epidural anesthesia to a "high-dose opioid" general anesthetic, including either fentanyl or sufentanil, significantly reduces catecholamine concentrations during and after bypass relative to concentrations measured without thoracic epidural anesthesia (28,29) (Fig. 17.5).
The effect of pulsatile perfusion on catecholamine concentrations during CPB remains controversial (16,30). Although early studies demonstrated that catecholamine concentrations were increased during bypass whether or not pulsatile perfusion was used (16), a more recent study of elective coronary surgery patients showed significant reductions in epinephrine and norepinephrine concentrations with pulsatile perfusion (30) (Fig. 17.6).
Some increase in catecholamine concentrations during and after bypass may be unavoidable with current anesthetic and surgical techniques; nevertheless, higher doses of opioids, inhaled general anesthetics, and epidural local anesthesia can limit the increases.


